
A 35 year old previously healthy female presents with right sided chest pain after a motorcycle crash. She describes the pain as worse with deep inspiration over her right anterior chest. Her vital signs are as follows: T 98°F (36.67°C) HR 110, BP 130/80, RR 18, 98% on RA. On examination she is mildly distressed with bilateral breath sounds, diffusely tender to palpation over her right anterior chest.
Bedside ultrasound of patient’s lungs is performed and demonstrates the following:
What do the images show? What is the diagnosis? (Click the button for the answer!)

Unilateral B-lines consistent with pulmonary contusion.
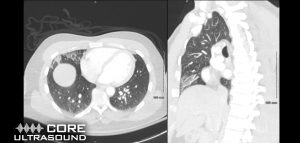
This ultrasound demonstrates focal B lines isolated to the patient’s right upper and middle lung. Pneumothorax can be ruled out by the presence of B lines with normal lung sliding.¹ B lines suggest increased density within the lung tissue, most commonly from fluid. They can be seen on ultrasound in several different disease processes; including pulmonary edema, pneumonia, and pulmonary contusion. 2 Additional findings that can be seen with pulmonary contusions include pleural line abnormalities and subpleural consolidations.3,4 In the context of this patient’s traumatic injury, isolated B lines represent pulmonary contusion. The patient received a CT scan of her chest (seen blow), confirming the diagnosis, and was subsequently admitted for supportive care and observation.
Pearls:
- Pulmonary contusions are the most common lung injury in patients with blunt chest trauma, with an incidence of roughly 25%.3
- They often occur from compression-decompression injuries such as high speed MVC’s, which cause direct injury to the lung parenchyma with resulting hemorrhage and edema.4
- Diagnosis can be made with bedside ultrasound by using the curvilinear probe and identifying the presence of focal B lines, pleural line abnormalities, and subpleural consolidations. 2,3
- The presence of B lines has near 100% sensitivity of ruling out pneumothorax. 1
- Sensitivity and specificity for diagnosis of pulmonary contusion on lung ultrasound is 92% and 89%, respectively. In the same study, chest radiography was found to be 44% sensitive and 98% specific. Therefore, ultrasonography is a superior screening method than conventional chest radiography for pulmonary contusion.6
- The treatment of pulmonary contusion involves maintenance of adequate ventilation and pain control.5
- Early diagnosis is key as many patients are at high risk of developing subsequent pneumonias or ARDS.3,4
Case Courtesy of Jack Yancey, MD
Case Written by Jacob Avila, MD
References
- Soldati G, Sher S, Copetti R. If you see the contusion, there is no pneumothorax. Am J Emerg Med. 2010; 28(1):106-7; author reply 107-8. [PMID: 20006213]
- Soldati G, Sher S, Testa A. Lung and ultrasound: time to “reflect”. Eur Rev Med Pharmacol Sci. 2011; 15(2):223-7. [PMID: 21434491]
- Stone MB, Secko MA. Bedside ultrasound diagnosis of pulmonary contusion. Pediatr Emerg Care. 2009; 25(12):854-5. [PMID: 20016357]
- Soldati G, Testa A, Silva FR, Carbone L, Portale G, Silveri NG. Chest ultrasonography in lung contusion. Chest. 2006; 130(2):533-8. [PMID: 16899855]
- Jones D, Nelson A, Ma OJ. Pulmonary Trauma. In: Tintinalli’s Emergency Medicine A Comprehensive Study Guide. 8th ed. McGraw-Hill Education; 2016:1744-1746.
- Hosseini M, Ghelichkhani P, Baikpour M, et al. Diagnostic Accuracy of Ultrasonography and Radiography in Detection of Pulmonary Contusion; a Systematic Review and Meta-Analysis. Emerg (Tehran). 2015;3(4):127–136.
